Cooperation with Dr. Ulf Kessler in Lausanne
Visceral surgeon Dr. Ulf Kessler has been at Hirslanden Clinique Cecil as an attending physician for more than a year, and has his practice at CMD Lausanne. With his extensive experience in visceral surgery, he is a competent partner for Swiss1Surgery with Dr. Jörg Zehetner, Professor (USC), in the special field of reflux surgery, as well as surgical intervention with the LINX Reflux Management System.
With the cooperation of Dr. Ulf Kessler and Swiss1Chirurgie, the range of services for the use of the LINX Reflux Management System can now also be offered in Lausanne. In this way, we are extending our radius of action to western Switzerland in the interests of our patients.
In March 2022, the collaboration between Dr. Jörg Zehetner and Dr. Ulf Kessler successfully treated a patient with the LINX Reflux Management System for the first time at the Hirslanden Clinique Cecil in Lausanne. The 45-minute operation was minimally invasive and the patient was discharged from the hospital after two days without any symptoms.
What’s new?
Dr. Zehetner has already performed 350 surgeries with the LINX Reflux Management System in Bern since 2015. This surgery is considered for all patients with typical reflux symptoms, small to moderate diaphragmatic hernia and with normal esophageal function. Now this surgical technique, which has been tried and tested worldwide for ten years, is also available to patients in French-speaking Switzerland.
With Dr. Ulf Kessler, an ideal partner for such interventions was found. Dr. Ulf Kessler was in training for a period of three years to specialize in visceral surgery at the Hirslanden Klinik Beau-Site in Bern, and has already worked with Dr. Jörg Zehetner – as the responsible tutor for Upper GI Surgery and Bariatric Surgery.
During this time, the results of the first 150 operations with the LINX system were also published in Bern. Dr. Kessler’s scientific collaboration was a key factor in the success of the project. In the Hirslanden Center for Digestive Diseases in Lausanne, an ideal partner was found for Western Switzerland, especially since important accompanying specialties such as endoscopy and gastroenterology/hepatology are also on site there.
Interested patients and affected relatives from Western Switzerland can contact Dr. Kessler directly in the future. With his team on site in Lausanne, Dr. Kessler will then perform the assessment and, in collaboration with Swiss1Surgery with Dr. Zehetner, perform any surgical procedures using the LINX Reflux Management System.
Through this collaboration, the good care during the clinic phase and also the follow-up by an experienced specialist can be guaranteed.
The cooperation between Swiss1Surgery and Dr. Ulf Kessler is groundbreaking for this field. This means that the expertise of Dr. Jörg Zehetner, who has the most experience with the LINX system in Switzerland to date, can also be made available to patients in French-speaking Switzerland.
For patients with special questions, the Swiss1Surgery practice in Bern and the GGP Gastroenterology Group Practice with its special functional diagnostics naturally remain a direct and good point of contact.
For further questions we gladly refer to the website www.swiss1chirurgie.ch


Reflux and oesophageal cancer – An inside view
Vom 21. bis 27. November 2021 läuft die GERD Awareness Week. GERD steht für Gastroesophageal Reflux Disease, also kurz gesagt die Refluxkrankheit. Betroffen davon sind etwa 20 Prozent der Bevölkerung. Das individuelle Erscheinungsbild und Ausmass kann dabei sehr unterschiedlich ausgeprägt sein. Wir wollen anlässlich der GERD Awareness Week den Blick auf die Refluxkrankheit, mögliche Folgeerkrankungen und eine zielgerichtete Diagnose und Behandlung richten. Dabei ist uns die ganz persönliche Sicht Betroffener ebenso wichtig wie die Möglichkeiten der chirurgischen Intervention und die Chancen der Vorsorge und gezielter Nachsorge.
Saures Aufstossen ist mehr, als nur unangenehm
Im Rahmen der GERD Awareness Week setzt die Swiss1Chirurgie noch einmal verstärkt auf die Aufklärung zu Refluxerkrankungen, die sich oftmals durch chronisches saures Aufstossen ankündigen oder bereits vorliegen. Von der ersten individuellen Wahrnehmung über eine fachmedizinische Diagnostik bis hin zur chirurgischen Intervention reicht die Spannbreite der Wahrnehmung von Refluxerkrankungen, die zumindest in bestimmten Bevölkerungsgruppen weiter auf dem Vormarsch sind. Mehr zum Thema lesen Sie im Beitrag.
Saures Aufstossen, die persönliche Sicht
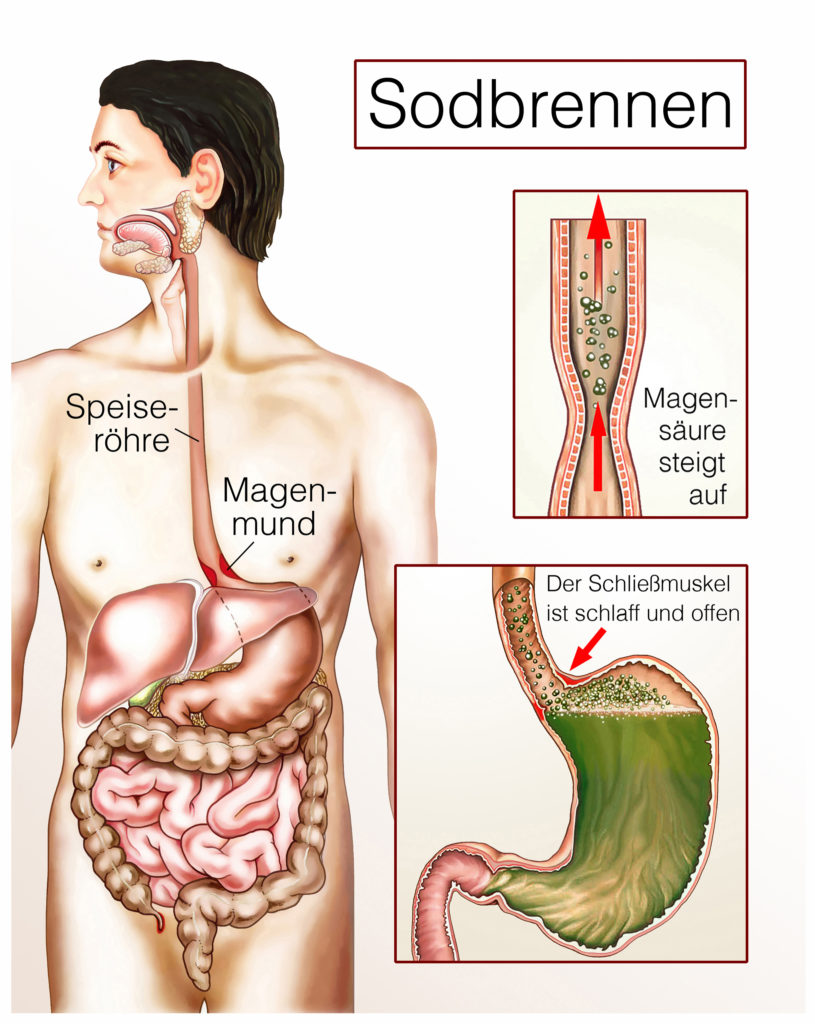
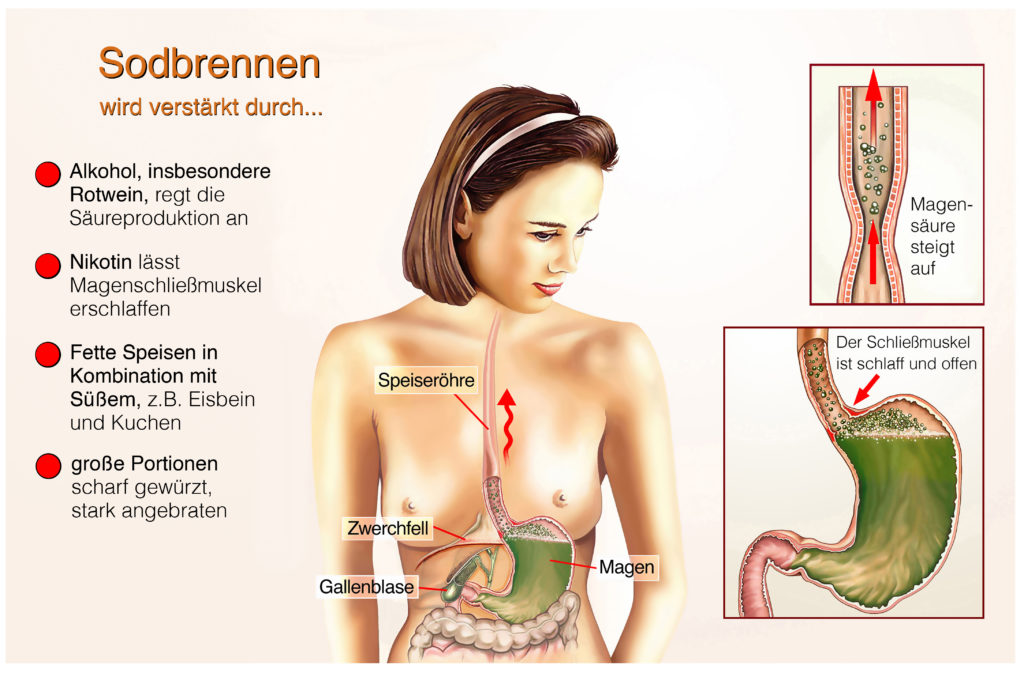
Upps, da ist es wieder. Dieses unangenehme Aufstossen von saurem Magensaft mit diesem bekannt widerlichen Gefühl. Magenflüssigkeit und im Einzelfall auch Nahrungsbestandteile steigen vom Magen in die Speiseröhre auf und sorgen neben dem bitteren Beigeschmack für ein Gefühl des Unwohlseins. Besonders nach üppigem, fettreichen oder scharfen Essen klagen viele über das sogenannte Sodbrennen, machen sich aber wenig Gedanken, darüber, wo die Ursachen zu suchen sind und welche Folgeerscheinungen möglich sind. Übrigens tragen auch Alkoholkonsum, deutliches Übergewicht und das Rauchen zur Ausbildung und Verstärkung von Refluxerkrankungen bei. Richtig lästig wird es, wenn dieses saure Aufstossen immer häufiger und wiederkehrend auftritt. Dann reden wir bereits vom chronischen Aufstossen, das durchaus Krankheitswert haben kann. In der Endkonsequenz wird es wichtig sein, jetzt einen versierten Mediziner zu finden, der sich mit der Diagnose, Behandlung und Nachsorge der Refluxkrankheit tatsächlich gut auskennt. Der erste Weg ist dann meist der zum Hausarzt, der dann als Zuweiser die passenden Fachmediziner finden sollte. Wichtig ist in jedem Fall, chronisches saures Aufstossen nicht auf die leichte Schulter zu nehmen, sondern frühzeitig die fachmedizinische Sicht einzuholen. Denn aus anfangs gelegentlichem Aufstossen kann schnell mehr werden, mit entsprechend schwerwiegenden Folgen.
Wenn aus chronischem Aufstossen Krebs wird, die medizinische Sicht
Der Weg vom chronischen Aufstossen bis zum Speiseröhrenkrebs ist in vielen Fällen kürzer, als gemeinhin angenommen. Durch den wiederholt in der Speiseröhre aufsteigenden Magensaft wird die empfindliche Schleimhaut der Speiseröhre angegriffen und ernsthaft geschädigt. Im weiteren Verlauf entwickeln sich Zellwachstumsstörungen, die im Ernstfall zu unkontrolliertem Zellwachstum und damit zu Speiseröhrenkrebs führen können.
In einem frühen Stadium spürt der Patient davon kaum etwas, sodass nur eine zeitige medizinische Diagnose und Intervention Aufschluss bieten und eine adäquate Behandlung sicherstellen kann. Ist die Speiseröhre bereits stark geschädigt und ein deutliches Krebswachstum vorhanden, äußert sich das bei den Patienten durch deutliche Schluckbeschwerden und gegebenenfalls auch mit einem Druckgefühl im Brustbereich, dass vom Patienten selbst jedoch kaum klar lokalisiert werden kann. Hier ist dann dringlichst eine fachmedizinische Diagnose erforderlich, um eventuell noch rechtzeitig eingreifen zu können. Ein Hinwarten verbessert die Situation nicht, sondern führt eher zu einer verschlimmerten Gesamtsituation.
Daher ist es in jedem Fall von gehäuftem sauren Aufstossen ratsam, baldigst einen Fachmediziner aufzusuchen, um im diagnostischen Prozess die konkrete Lage und eine eventuelle Gefährdungssituation professionell abschätzen zu können. Mit handelsüblichen Präparaten gegen Sodbrennen lässt sich der Prozess zwar mildern, aber nicht effektiv aufhalten oder beenden.
Chirurgische Intervention, der notwendige Eingriff
Ist ein chirurgischer Eingriff bei einer Refluxerkrankung erforderlich, dann greifen die Experten der Swiss1Chirurgie bevorzugt auf minimalinvasive Operationsmethoden zurück. Dabei wird nicht am Symptom, sondern an der Ursache angesetzt. Die Ursache für das chronische saure Aufstossen ist häufig am Übergang zwischen Speiseröhre und Magen und oftmals auch im Durchgangsbereich am Zwerchfell zu suchen. Das, nennen wir es Ventil am Mageneingang schliesst nicht mehr richtig oder ist in seiner Funktion anderweitig beeinträchtigt, so dass immer wieder saurer Magensaft nach oben steigen kann. Nicht selten ist auch die Pumpfunktion der Speiseröhre gestört, was sich in einem Funktionstest ermitteln lässt.
In der Swiss1Chirurgie wird nach Möglichkeit ein System eingesetzt, bei dem ein elastischer Magnetring um das Speiseröhrenventil gelegt wird. Dieser Magnetring verschliesst den Übergang von Speiseröhre zum Magen, erlaubt aber das normale Aufnehmen von Nahrung, sofern der Druck in der Speiseröhre normal ist. Auch ein leichtes Aufstossen von Luft bleibt möglich.
Über dieses Verfahren und andere Möglichkeiten der Behandlung von Refluxerkrankungen können Sie sich umfassend und komfortabel auf unserer Webseite informieren.
Gefährdete Gruppen und Tendenz
Von Refluxerkrankungen sind vor allem Menschen betroffen, die Schwächungen am Übergang von der Speiseröhre zum Magen aufweisen. Eine grosse Gruppe der Patienten rekrutiert sich aus der Gruppe der übergewichtigen Menschen. Wenngleich das nicht das alleinige Risiko abbildet, ist Übergewicht doch ein entscheidender Faktor bei Refluxerkrankungen. Auch übermässig fettes und scharfes Essen provoziert Refluxstörungen ebenso wie der übermässige Alkoholkonsum oder das Rauchen.
Tendenziell kann davon ausgegangen werden, dass Refluxerkrankungen weiter zunehmen werden. Ursache dafür sind das Ernährungsverhalten der Menschen und der übermässige Gebrauch von Genussmitteln. Eine insgesamt gesunde Lebensweise kann auch Refluxerkrankungen vorbeugen, wenngleich auch anscheinend gesund lebende Menschen davon betroffen sein können.
Was zu tun bleibt
Wer bereits über Refluxbeschwerden klagt, sollte insbesondere sein Essverhalten überprüfen. Fettiges Essen, grosse Portionen, saures und scharfes Essen sollten ebenso vermieden werden wie ein Zuviel an Kaffee, Schokolade, Alkohol und Nikotin. Eine Gewichtsreduktion ist in vielen Fällen ratsam.
Sollten sich auch dann keine kurzfristigen Verbesserungen einstellen, ist der Gang zum Hausarzt oder direkt zum Experten für Refluxerkrankungen unerlässlich. Nur dort kann die Situation klar und eindeutig abgebildet werden, was schlussendlich der sicherste Weg zu einer zutreffenden Diagnose und einer nachfolgenden Behandlung ist.
Auch zu den Möglichkeiten der Beeinflussung von Refluxerkrankungen finden Sie auf unserer Webseite umfangreiches Material.
Für Fachkollegen empfehlen wir die Teilnahme am Zuweiserevent am 25. November 2021 im Rahmen der GERD Awareness Week 2021.
Belching, obesity and diabetes – recognising connections
At the 4th Helvetius Holding AG symposium, Dr. med. Jörg Zehetner, Professor (USC), dealt with the connection between reflux diseases, obesity and diabetes in a detailed lecture. In most cases, there are causal relationships between the different clinical pictures, which must also be taken into account in medical therapy. While a large proportion of overweight patients also complain of reflux, the links between obesity and diabetes are even more apparent. Both diseases are reciprocal consequences and triggers of the other disease. This also affects the professional approach to therapy. The full article on the lecture, a video stream of the lecture and further information can be found here.
In his highly acclaimed lecture at the 4th Helvetius Holding AG symposium at the Talent Campus Bodensee in Kreuzlingen, Dr. med. Jörg Zehetner, Professor (USC), revealed the connections between belching, obesity and diabetes. Based on the latest scientific findings and from his own medical clinic, Dr. med. Jörg Zehetner has developed a model from this that makes it clear how the connections are to be seen, which health restrictions and experiences result from this and which medical interventions are indicated.
Dr. med. Jörg Zehetner is considered THE specialist in visceral and obesity surgery in Switzerland. His comprehensive training and specialisation also make him a sought-after specialist abroad, for example as a supporting luminary to his professional colleagues in the United Arab Emirates. The extended training in the USA and his own scientific research have made Dr. med. Jörg Zehetner a proven specialist in his field. As the head of one of the largest private practices in Switzerland, he is the head of Swiss1Chirurgie and offers patients, their relatives and specialist colleagues a wide range of modern treatment methods and expanded options for therapy in the association of companies that operate under the umbrella of Helvetius Holding AG.
Individual clinical pictures, diagnoses and complaints are often closely linked and not infrequently form a kind of causal reaction chain in which one abnormality causes the other or is a consequence of previous illnesses. Therefore, it is important to look for and find the possible connections between different symptoms.
The clinics in the Helvetius Holding AG network
First, a few introductory words about Swiss1Chirurgie. The Swiss1Chirurgie is a visceral surgery clinic in which Dr. med. Steffen, Dr. med. Anita Scheiwiller, Dr. med. Metzger, Dr. med. Flückiger, Dr. med. Fringeli and Dr. med. Jörg Zehetner provide highly specialised medical services for patients. The Swiss1Chirurgie sites are in Bern, in Solothurn and in Valais, where patients are treated primarily in the specialties of bariatrics, reflux diseases, oesophageal and stomach cancer, colon, thyroid diseases, liver diseases and hernias.
The Centre for Bariatric Surgery ZfbC has established itself as a specialised pre- and post-operative care centre for bariatric surgery in conjunction with Swiss1Chirurgie. Here, patients are cared for holistically by the specialists before a necessary operation and after the surgical procedure.
The Gastroenterology Group Practice Bern GGP is the centre for endoscopic examinations and functional diagnostics. Chronic diseases of the gastrointestinal tract are also treated here.
An internal medicine clinic has established itself in the Bern PZBE clinic and offers services here not only in the field of internal medicine, but also in the special field of psychosomatics.
All specialist practices under the umbrella of Helvetius Holding AG are staffed with experienced medical specialists, work closely with each other and thus provide holistic and professional healthcare and necessary medical interventions in the overall concert of specialist medical services for the benefit of patients.
Reflux – Acid regurgitation
Everyone is certainly familiar with acid regurgitation, for example after a sumptuous and very fatty meal or after excessive alcohol consumption. An occasional belching with clearly defined temporary symptoms is not a problem at first.
Acid reflux only becomes a problem if it occurs chronically, i.e. more or less repeatedly, and if it is actually disturbing or even annoying to the body. Then we are talking about reflux. By reflux we mean that gastric juice rises from the stomach into the oesophagus. The stomach acid not only leads to the familiar unpleasant sour sensation, but in its chronic form can also lead to serious burns of the oesophagus and even to the development of oesophageal cancer.
The whole thing is referred to in medical parlance as Gastroesophageal Reflux Disease, or GERD for short, and is a serious disorder with disease value. This is a disease of the sphincter and/or diaphragm, but is favoured by other factors. One of the factors that cause gastric juice to be expelled into the oesophagus is a valve at the junction between the oesophagus and the stomach that does not function normally. Normally, this valve prevents acidic gastric juice from being pushed up into the oesophagus. If the function of this valve is disturbed, reflux can occur. This valve is located at the transition from the thorax to the abdominal cavity, which is practically formed by the diaphragm. The oesophagus runs through the diaphragm.
A normal function of the valve requires that this valve itself is organically completely without findings. Furthermore, a normal weight is a good prerequisite for the undisturbed functioning of the valve. If you are overweight, the increased pressure on the abdomen and diaphragm alone means that the function of the valve can be restricted. The mechanism works in such a way that the lungs pull in normal function, while an overfull abdomen pushes against it, so that the function of the valve is affected in only one direction, upwards. As a result, a defective or weak valve at the transition from the oesophagus to the stomach allows gastric juice to flow back.
It should be noted that the stomach does not only contain gastric acid. Pepsin, bile, pancreatic juice and of course food components in variously decomposed forms are found in the stomach. If the pumping function of the oesophagus is disturbed and the valve is not fully functional, all these components are pressed into the oesophagus, which is not only unpleasant but can also become really dangerous in the long term.
Treatment of reflux disease
Reflux can be treated conservatively in many cases. A change in lifestyle is just as helpful as a diet. Avoid spicy foods, coffee, greasy and fried foods, onions, garlic and tomatoes, fruits and fruit juices. Furthermore, dark chocolate with a high cocoa content, alcohol, carbonated drinks, large food portions and, in individual cases, certain medicines should be avoided.
Often, avoiding such factors already helps to reduce reflux. It is remarkable that smokers complain more about reflux, as smoking also has a loosening effect on the function of the valve described above. The same applies to other stimulants, which we have described here before with dark chocolate and alcohol.
When changing our lifestyle, the most important thing is that we don’t always eat the really big portions, but rather smaller portions more often. Opulent food right before going to bed should also be avoided. There are a number of medications that affect the function of the oesophago-gastric valve. A whole industry has grown up around acid reflux, which often sells its medicines without a prescription, virtually at discount stores.
The function of such medicines is usually only oriented towards the symptom, but not the cause. Such medicines do not stop the actual reflux, but reduce the production of stomach acid. They are nothing more than so-called acid blockers, but have no effect on the production of bile, pepsin or pancreatic juices and have no effect whatsoever on the defective or weakened valve at the junction between the oesophagus and the stomach. Therefore, the mode of action always remains limited and ultimately does not change the causes of reflux.
This means that only a part of the whole symptomatology, i.e. the stomach acid, is removed or reduced, but the problem as such remains.
Reflux surgery
Until ten years ago, only two procedures were actually established for reflux. On the one hand the Nissen fundoplication and on the other hand the Toupet fundoplication. While good oesophageal function is a prerequisite for the Nissen fundoplication, the Toupet fundoplication can also be used in cases of poor oesophageal function.
At Swiss1Chirurgie, we have been using the LINX system in the therapeutic treatment of reflux in Switzerland since 2015. In simple terms, this LINX system is a magnetic ring made up of individual parts on a kind of belt. This magnetic band closes the transition between the oesophagus and the stomach, but opens under a certain pressure so that, on the one hand, normal food intake into the stomach but, on the other hand, vomiting remains possible. However, the relatively light pressure of reflux is stopped so that no gastric juices can push up into the oesophagus.
Another advantage of this system is that a normal diet is possible postoperatively and air can also be expelled, which is not to be expected with the older procedures. Furthermore, when using the LINX system, there is significantly less of the feeling of fullness known from the other methods and no increased flatulence.
As part of a medical study, we have also been using RefluxStopTM in Swiss1Chirurgie since 2020. This involves fixing the stomach to the oesophagus in order to maintain the lower sphincter in the abdomen. A small silicone ball holds the prepared area in position, allowing an almost natural situation to be restored. In all such operations, the existing diaphragmatic hernia must also be treated surgically.
Jörg Zehetner, MD, is the only surgeon in Switzerland to offer his patients all of the procedures listed here. He always makes his decisions individually and on the basis of the situation found in the individual case. The important starting point for the decision is the function of the oesophagus. With normal oesophageal function, the LINX system and the Nissen fundoplication can be used well. In cases of moderately to severely reduced oesophageal function, the Toupet fundoplication, the RefluxStopTM system or, in exceptional cases, a Dor fundoplication are more likely to be used. In the clear majority of cases, the proven LINX system can be used.
Problems due to reflux
In addition to the actually already unpleasant appearance of reflux due to the repeated acid regurgitation, reflux also hides clearly dangerous constellations. The constant acid attack on the inner oesophagus often leads to infectious processes. These infections can lead to changes in the oesophageal mucosa. As a result, the mucous membrane changes in such a way that at some point it also shows tissue changes that are visually very reminiscent of stomach tissue. Such tissue then also has the potential to develop cancer. So oesophageal cancer cannot be ruled out and is always on the cards as it progresses. This is not something to be taken lightly. Adequate treatment is urgently needed.
The statistical evaluation shows that oesophageal cancers have increased significantly since 1975. Here, an increase of 700 percent can be observed in the last 30 to 40 years. For men, it is the cancer that has increased the most worldwide.
If we look at the correlations between reflux, obesity and diabetes in the following, some correlations become clear even in the statistical analysis.
Connection between overweight and reflux
In general, it can already be stated here that the probability of suffering from reflux increases significantly with the presence of severe overweight. For example, the body mass index BMI was compared and correlated with acid exposure. A BMI of 30 or more is referred to as obesity, which is expressed in various classifications. A BMI of 35 or more can be considered pathologically overweight.
Being morbidly overweight is not just a matter of external symptoms such as a colloquial “beer belly” and the inevitable fat deposits. With a BMI over 40, we already speak of a metabolic syndrome, which can be defined by diabetes, high blood pressure, elevated cholesterol levels, fatty liver, high blood fat levels as well as arthritis and gout.
These symptoms also increase the risk factors for cardiovascular disease, stroke, sleep apnoea, cancer, abdominal wall hernias and reflux disease. The risk of oesophageal cancer then increases again with the reflux diseases. This observation already shows that the connections and transitions between reflux, obesity and diabetes must be considered causally.
When assessing the development of obesity, the tendency is that obesity is increasingly observed worldwide, especially in the developed industrialised countries but even in the developing countries. And this is happening at a breathtaking rate of progression in close connection with a food oversupply with virtually unlimited availability of food.
As body weight increases, it is not only the outwardly visible fat deposits that occur. The liver is always particularly affected, which develops from a healthy liver to a fatty liver and even cirrhosis with increasing obesity. On the topic of fatty liver, we have provided a separate contribution and lecture by Dr. med. Michaela Neagu from the Gastroenterological Group Practice Bern GGP. A contribution and lecture by Dr. Hardy Walle on liver fasting is also available.
If you look at the phenomena of obesity with a close look at the metabolic processes in the body, then a concrete connection to diabetes can also be established. If you bring together the statistical data on obesity and diabetes, the interaction becomes more than clear.
It should also be clearly assessed that a fatty liver is often the cause of diabetes, but diabetes can also be the cause of a fatty liver. Here, a kind of vicious circle closes that can only be broken by appropriate medical interventions.
The function of the pancreas is clearly related to diabetes. The pancreas lies anatomically behind the stomach and fulfils two essential functions. On the one hand, it supports the digestive function, on the other hand, it produces insulin, which is required for the metabolisation of sugar, more precisely glucose. Insulin affects the sugar balance in the liver, fatty tissue and muscles. In overweight people, this metabolism is disturbed. The fatty cells show resistance to insulin uptake, which significantly disturbs the metabolisation of glucose. As a result, blood glucose levels deviate from normal. Progressive diabetes mellitus develops.
Diabetes mellitus is divided into two types. Type 1 with subgroups 1a and 1b. Diabetes mellitus type 1a is mostly observed as a congenital form in childhood and manifests after viral infections.
Type 1b is seen up to about 35 years of age and is associated with islet cell antibodies and autoimmune system disorders.
Diabetes mellitus type 2 used to be called adult-onset diabetes and occurs mainly in overweight people with a disturbed metabolism. In the meantime, we are increasingly observing diabetes mellitus type 2 also in children and adolescents who are very overweight. Type 2 diabetes mellitus is even more common in children and adolescents than type 1.
The problem with diabetes is not only the damaged metabolism. The blood vessels, liver and heart function are also affected. Arteriosclerosis often occurs, leading to narrowing or blockage of blood vessels. The risk of heart attack increases fivefold and the risk of stroke triples.
The course of diabetes is a progressive process that initially appears to be easily manageable, but as it progresses, it requires more and more specialist medical intervention. In the context of diabetes and obesity, it has been shown that surgically treated obesity patients often experience a better and faster improvement in diabetes than those with only drug treatment. Of course, if the obesity surgery is done after many years of an existing diabetes, the likelihood that the diabetes will also improve again is reduced.
Accordingly, it is important not to put off obesity surgery for a long time in patients with a BMI of 40 or more when diabetes is just beginning. The sooner action is taken, the greater the effects both on body weight and on preventing the progression of diabetes.
It is important to understand that obesity is a disease and must be treated as such. Different studies clearly show that in cases of severe obesity, obesity surgery is always the better solution compared to other medical interventions, also with an effect on diabetes.
Effects of metabolic surgery
If all experiences from metabolic surgery are considered in the context of reflux, obesity and diabetes mellitus, the following effects can be demonstrated in patients with a BMI over 40:
- generally improved quality of life
- greater improvement in blood glucose levels
- Reduced consumption of diabetes medication
- fewer vascular diseases
- fewer strokes
- reduced cancer risk
- Less overall mortality
- Higher weight loss than with conservative therapies
Only two to three percent of patients with a BMI over 40 achieve significant weight reduction in conservative therapies. Only patients with a BMI between 30 and 35 often show good results with conservative therapies.
View bariatric surgery as a whole
Bariatric surgery presents itself as a triad that does not stop at one surgical procedure. The operation alone does not solve the problem. Important is the interaction of
- Lifestyle change
- Change in dietary habits and
- surgical intervention with good pre- and aftercare
Modern surgical procedures have long since bid farewell to the gastric banding that has been used for many years. In the USA and Germany, the preferred outcome of the operation is the formation of a tube stomach. This affects up to 60 percent of patients. In Switzerland, the current level here is around 30 percent. Partial removal of the stomach also achieves hormonal effects, as the passage of food through the stomach is accelerated and the small intestine is much more likely to be activated with corresponding hormone release.
Another option is gastric bypass, which is performed laparoscopically. This technique is preferably used in patients with pre-existing diabetes or pre-existing reflux. With a share of about 70 per cent, this is the most frequently performed bariatric operation in Switzerland. A small gastric pouch is formed and connected directly to the small intestine.
Additional information
You can watch the entire lecture in its original wording, with additional questions and answers as well as interesting statistics here in the stream.
In addition, we recommend further articles and videos that were produced as part of the Helvetius Holding AG symposia.
What is LINX, what can LINX do?
Swiss1Chirurgie informs – The LINX System
Constant acid regurgitation is not only annoying, but can also cause serious secondary diseases. What is summarised in technical language as reflux is an extremely unpleasant restriction of the quality of life for those affected.
The LINX system has been available for years for reflux therapy and has led to extremely positive results. You can find out what LINX is, what LINX can do and how it works in the detailed article, in the video or on the Swiss1Chirurgie website.
Learn more about the reflux therapy procedure
There are probably around 20 percent of the population who regularly or chronically complain of reflux of stomach acid into the oesophagus. However, acid regurgitation is not only extremely unpleasant, but can also cause serious health problems, including oesophageal cancer.
With LINX, a system is available that can effectively prevent the backflow of gastric juice into the oesophagus. This system is used as part of a minimally invasive surgical operation. After placement of the LINX system, the symptoms subside and patients can return to a normal life in most cases.
What is LINX?
In principle, the LINX system is a magnetic ring chain. At first glance, the system can be compared to an elastic pearl necklace, whereby here the pearls are on magnets that are titanium-coated and thus completely harmless to the organism. Due to the attractive forces acting on the magnetic beads, they are repeatedly attracted to each other in the absence of counterpressure, which leads to a narrowing of the chain. When mechanical tension is applied to the system, the chain expands and widens the passage.
What can LINX do?
The LINX system is placed around the lower end of the oesophagus in a minor surgical procedure. The attraction of the titanium-coated magnetic beads creates a reliable closure of the oesophageal outlet without compressing the oesophagus. Only when, for example, a certain internal pressure is exerted on the oesophagus by the intake of food, does the magnetic ring open so that the food pulp or even liquids can enter the stomach unhindered. In this way, the normal function of the oesophagus is efficiently supported and the reflux of gastric juice into the oesophagus can be prevented. The bottom line is that LINX is strong enough to close the oesophageal junction into the stomach, but weak enough to allow air to escape from the stomach or vomiting to occur.
Practical experience
The LINX system has been known and proven for years. In the Swiss1Chirurgie clinics, this system is preferably used for reflux therapy whenever possible. The experience is extremely good, which includes that there are hardly any complications with the system during and after the surgical procedure. Since 2015, Prof. Dr. Jörg Zehetner has already treated over 250 patients with the LINX system. For most people with reflux symptoms, this system is the first choice, provided there is otherwise normal oesophageal function.
In order to assess this condition, a preliminary assessment of oesophageal function and reflux symptoms is essential. This preliminary examination includes a gastroscopy and a functional test of the oesophagus. Ideally, these examinations are supplemented by manometry, which means measuring the pressure in the oesophagus.
Would you like more information? Do you yourself have complaints due to acid reflux? Then watch the video with Prof. Dr. Jörg Zehetner, visit the Swiss1Chirurgie website or make an appointment at one of the Swiss1Chirurgie clinics in Bern, Brig or Solothurn.
OESOPHAGECTOMY: THE TREATMENT OF OESOPHAGEAL CANCER
By DR. MED. JÖRG ZEHETNER, Professor (USC), Specialist in Surgery, esp. Visceral surgery
EVERY YEAR, AROUND 600 PEOPLE IN SWITZERLAND ARE DIAGNOSED WITH OESOPHAGEAL CANCER. MEN ARE PARTICULARLY AFFECTED, ACCOUNTING FOR THREE QUARTERS OF ALL CASES, AND ARE SIGNIFICANTLY MORE LIKELY TO FALL ILL THAN WOMEN. WE EXPLAIN TO YOU WHAT OESOPHAGECTOMY IS ALL ABOUT. REFLUX DISEASE IS THE BIGGEST RISK FACTOR FOR OESOPHAGEAL CANCER.
https://v.calameo.com/?bkcode=006115199b76ca4b1be03&mode=mini&showsharemenu=false&clickto=embed
Successfully treat oesophageal cancer
If we analyse the cases of oesophageal cancer in Switzerland, we find that around 600 people suffer from this serious disease every year. The main risk for the development of oesophageal cancer are reflux diseases, which clearly favour the development of cancer in the oesophagus due to the pathological acid regurgitation. About three quarters of those affected are men. One of the promising therapies for oesophageal cancer is oesophagectomy, which will be explained in more detail in this article.
More information and interesting insights directly from Prof. Dr. med. Jörg Zehetner can be experienced in a Zoom Online lecture. Date: 10 March 2021, 6:30 pm to 7:30 pm.
Let’s start by explaining the technical terms that are important for this topic
The medical term reflux refers to the backflow of gastric acid from the stomach into the oesophagus. In layman’s terms, this is described as acid reflux. The cause of the backflow of stomach acid into the oesophagus is a weakening of the muscle at the end of the oesophagus (cardia). In addition to the actual acid regurgitation, patients describe such things as frequent heartburn, burning in the chest area or also stomach burning.
The oesophagus is called the oesophagus in medical vocabulary. Functionally, the oesophagus is a kind of muscular tube that transports food into the stomach through contractions. In the stomach, stomach acid, among other things, is responsible for breaking down the food as part of the digestion process. To protect the oesophagus from the constant acid attack, there is a muscle at the bottom of the oesophagus that closes it when it is functioning normally. If the function of this muscle is impaired, the reflux described above occurs.
In medicine, resection is the surgical removal of an organ or part of an organ. With reference to our topic, oesophagectomy is accordingly the surgical removal of the largest part of the oesophagus.
The risk factors for the development of oesophageal cancer
Over the years, the main risk factors for developing oesophageal cancer have changed somewhat. Whereas in the past it was smoking and excessive alcohol consumption, today it is persistent (pathological) acid regurgitation and obesity that significantly increase the risk of oesophageal cancer. If you follow the relevant advice books, acid blockers and diets are often recommended to get the problem of reflux under control. However, this only addresses the individually noticeable phenomena, but not the cause. Therefore, the risk of developing oesophageal cancer remains in the medium and long term unless the causes of acid regurgitation are consistently addressed. What remains is the no longer correctly functioning “valve” at the end of the oesophagus, i.e. the muscle that prevents the stomach acid from rising into the oesophagus. If no improvement can be achieved here, then the constant acid attack on the oesophagus ultimately threatens oesophageal cancer. Surgery on the reflux muscle at the right time can significantly reduce the risk.
From complaints to diagnosis
One of the most common complaints that bring patients to the doctor is difficulty swallowing. After anamnesis and a more detailed description of the symptoms, a gastroscopy is often performed. If malignant tissue is discovered or suspected in the oesophagus or at the transition to the stomach, it can be removed under a short anaesthetic using a type of mini forceps. A laboratory examination will confirm whether or not this is malignant tissue. In the former case, it must then be assumed that there is oesophageal cancer, which must be treated surgically as a matter of urgency. Once the diagnosis of oesophageal cancer has been made, the decision for a suitable therapy must be made.
Recommendation: Combined therapy
Before therapeutic steps are taken, the severity of the disease and the spatial spread of the oesophageal cancer must first be examined more closely and determined in detail. Computer tomography (CT) of the chest and abdomen is the method of choice for this. In this way, it is also possible to assess whether there are deposits in the lungs and liver. An ultrasound scan of the oesophagus can also assess deposits in the lymph glands.
A common feature of the work of the medical specialists at Swiss1Chirurgie and at the Beau-Site Clinic is an interdisciplinary tumour board, where specialists from all the disciplines involved carry out a precise assessment of the symptoms, risks and treatment options. In addition to recommending therapeutic measures, this also includes timely clarification of follow-up treatment.
In most of the cases, a combined therapy is considered by the tumour board. This combination consists of an upstream chemotherapy, which is to be understood as a preparation for the actual surgical intervention within the scope of the oesophageal resection. If necessary, radiotherapy can also be part of the treatment. The surgical intervention takes place a few weeks after the start of chemotherapy or radiotherapy.
The esophagectomy procedure
Thanks to modern surgical techniques, the removal of the oesophagus (oesophagectomy) can be performed as a minimally invasive procedure (also called keyhole surgery). The operation itself takes about three to four hours and is performed under anaesthesia. Through small incisions in the abdominal wall, the connections of the oesophagus to the stomach and at the diaphragm are loosened. The lymph glands in the abdomen are then removed, followed by removal of the oesophagus itself either through the abdomen or through the chest. The adjacent tissue, which may also be affected by tumour cells, is also removed.
In a further step, the stomach is formed into a tube. This stomach tube is finally connected to the upper remaining end of the oesophagus in the neck area. Afterwards, the success of the surgical procedure is checked using a method specially developed by Dr. Jörg Zehetner. For this purpose, a fluorescent substance is injected into the patient’s bloodstream. Within five to ten seconds, a laser camera can be used to determine whether the result of the operation is satisfactory.
Rapid mobilisation and recovery of patients
A clear advantage of modern surgical techniques in the context of oesophageal resection is the short time patients spend in hospital. With independent breathing, the operated patients wake up from the anaesthesia and remain in the intensive care unit for one to two days, depending on their condition, to monitor their bodily functions. In the normal ward, a swallowing X-ray is taken as early as five days after the operation to check whether the connection between the stomach tube and the beginning of the oesophagus has healed well. If this can be confirmed, the diet can be slowly built up.
Depending on the individual development, the clinic stay itself lasts about one week to ten days. This is followed by a two-week rehabilitation measure, which helps the patient to heal quickly. After just three months, the patient experiences his or her original quality of life, now without oesophageal cancer and the unpleasant accompanying symptoms. In principle, everything can now be eaten again, perhaps in smaller portions, but spread over several meals a day.
More information and interesting insights directly from Prof. Dr. med. Jörg Zehetner can be experienced in a Zoom Online lecture. Date: 10 March 2021, 6:30 pm to 7:30 pm.

Research for the benefit of patients
Swiss1Chirurgie accepts international award
When the specialists at Swiss1Chirurgie look for the best ways to treat patients, it always has a lot to do with research, scientific work and the publication of the latest findings and methods.
The doctors at Swiss1Chirurgie under Prof. Dr. Jörg Zehetner specialise in obesity surgery as well as medical treatments under the umbrella term UpperGI. This includes, for example, interventions in the areas of reflux, diaphragmatic hernias, oesophageal and stomach cancer. Another field of work of Swiss1Chirurgie is visceral surgery, which is also colloquially referred to as abdominal surgery. In all these specialties, the medical professionals not only work on the patients themselves, but also, and above all, in parallel in the areas of research and further development of methods and techniques.
International prize goes to Swiss1Chirurgie
While Prof. Dr Jörg Zehetner was still attending the OESO Congress in Beijing, Swiss1Chirurgie received a special honour. At the ASMBS Meeting 2019 in November in Las Vegas, USA, Dr Catherine Tsai received the International Award for the best video presentation of a surgical procedure.

Dr Catherine Tsai
Dr Catherine Tsai has been working as a research assistant at Swiss1Chirurgie in Bern for the past two years, and her scientific research work significantly supports further development at the Swiss1Chirurgie sites in Switzerland.
In the video presentation “Laparoscopic Conversion from Gastric Sleeve to RY Gastric Bypass with Remnant Gastrectomy using Fluorescent Angiography” by Dr Tsai, Dr Steffen and Dr Zehetner, you can see the laparoscopic conversion from a sleeve (tubular stomach) to a gastric bypass, whereby here the remaining stomach was completely resected for medical reasons. Fluorescent angiography was used to check the blood flow in the gastric pouch and duodenum, as shown in this video.
Swiss1Chirurgie continues its series of successes
The latest award ceremony for Swiss1Chirurgie and thus also for the Centre for Bariatric Surgery ZfBC continues a series of successes that have long since made the specialists Dr Jörg Zehetner, Dr Catherine Tsai, Dr Steffen and Dr Metzger real experts with an international reputation. We only need to refer to the numerous publications and prizes that were awarded to Swiss1Chirurgie last year.
The medical specialists are less concerned with fame and more with scientific, methodical and ultimately medical progress in the interest of the patients. Various studies are being carried out with the Inselspital Bern as well as in the Swiss1Chirurgie clinics and the Centre for Bariatric Surgery. The results of such studies primarily benefit the patients of Swiss1Chirurgie, underpin the outstanding international reputation of the specialists and, last but not least, form the basis for new developments in the specialist areas of Swiss1Chirurgie.
For the sake of completeness, we summarise here the most important publications, lectures and awards of Swiss1Chirurgie from the past years:
Swiss1Chirurgie accepts international award
When the specialists at Swiss1Chirurgie look for the best ways to treat patients, it always has a lot to do with research, scientific work and the publication of the latest findings and methods.
The doctors at Swiss1Chirurgie under Prof. Dr. Jörg Zehetner specialise in obesity surgery as well as medical treatments under the umbrella term UpperGI. This includes, for example, interventions in the areas of reflux, diaphragmatic hernias, oesophageal and stomach cancer. Another field of work of Swiss1Chirurgie is visceral surgery, which is also colloquially referred to as abdominal surgery. In all these specialties, the medical professionals not only work on the patients themselves, but also, and above all, in parallel in the areas of research and further development of methods and techniques.
International prize goes to Swiss1Chirurgie
While Prof. Dr Jörg Zehetner was still attending the OESO Congress in Beijing, Swiss1Chirurgie received a special honour. At the ASMBS Meeting 2019 in November in Las Vegas, USA, Dr Catherine Tsai received the International Award for the best video presentation of a surgical procedure.
Dr Catherine Tsai
Dr Catherine Tsai has been working as a research assistant at Swiss1Chirurgie in Bern for the past two years, and her scientific research work significantly supports further development at the Swiss1Chirurgie sites in Switzerland.
In the video presentation “Laparoscopic Conversion from Gastric Sleeve to RY Gastric Bypass with Remnant Gastrectomy using Fluorescent Angiography” by Dr Tsai, Dr Steffen and Dr Zehetner, you can see the laparoscopic conversion from a sleeve (tubular stomach) to a gastric bypass, whereby here the remaining stomach was completely resected for medical reasons. Fluorescent angiography was used to check the blood flow in the gastric pouch and duodenum, as shown in this video.
Swiss1Chirurgie continues its series of successes
The latest award ceremony for Swiss1Chirurgie and thus also for the Centre for Bariatric Surgery ZfBC continues a series of successes that have long since made the specialists Dr Jörg Zehetner, Dr Catherine Tsai, Dr Steffen and Dr Metzger real experts with an international reputation. We only need to refer to the numerous publications and prizes that were awarded to Swiss1Chirurgie last year.
The medical specialists are less concerned with fame and more with scientific, methodical and ultimately medical progress in the interest of the patients. Various studies are being carried out with the Inselspital Bern as well as in the Swiss1Chirurgie clinics and the Centre for Bariatric Surgery. The results of such studies primarily benefit the patients of Swiss1Chirurgie, underpin the outstanding international reputation of the specialists and, last but not least, form the basis for new developments in the specialist areas of Swiss1Chirurgie.
For the sake of completeness, we summarise here the most important publications, lectures and awards of Swiss1Chirurgie from the past years:
Swiss1Chirurgie Research Fellowship (2017-2019)
Conferences (number of presentations)
- International Federation for the Surgery of Obesity and Metabolic Disorders-European Chapter (IFSO-EC), Athens, Greece, May 2018 (3)
- European Association of Endoscopic Surgery (EAES), London, UK, May 2018 (2)
- Digestive Disease Week – Society for Surgery of the Alimentary Tract (DDW – SSAT), Washington DC, June 2018 (3)
- IFSO, Dubai, UAE September 2018, (4)
- American College of Surgeons (ACS), Boston, MA, October 2018 (2)
- SAGES, April 2019, Baltimore, MD (2)
- World Congress on Interventional Therapies for Type 2 Diabetes (WCITD), April 2019, New York, NY (1)
- DDW, May 2019, San Diego, CA (1)
- Swiss Surgical Society, May 2019, Bern, Switzerland (6)
- ASMBS Obesity Week, November 2019, Las Vegas, Nevada (2)
Publications (4)
- Tsai C, Steffen R, Kessler U, Merki H, Zehetner J, “Short-term outcomes of endoscopic gastro-jejunal revisions for treatment of dumping syndrome after Roux-En-Y gastric bypass,” Surgical Endoscopy, September 2019
- Tsai C, Zeheter J, Beel J, Steffen R, “Long-term outcomes and frequency of revisional bariatric surgeries beyond 15 years after gastric banding: A high band failure rate with safe revisions,” SOARD, February 2019
- Tsai C, Kessler U, Steffen R, Merki H, Zehetner J, “Endoscopic Gastrojejunal Revisions Following Gastric Bypass: Lessons Learned In More Than 100 Consecutive Patients,” Journal of Gastrointestinal Surgery, September 2018
- Tsai C, Kessler U, Steffen R, Merki H, Zehetner J, “Endoscopic Closure of Gastro-gastric Fistula After Gastric Bypass: a Technically Feasible Procedure but Associated with Low Success Rate,” Obesity Surgery, September 2018
Oral Presentations (16)
- Tsai C, Steffen R, Zehetner J, “Magnetic Sphincter Augmentation for Treatment of Gastroesophageal Reflux Disease after Roux-En-Y Gastric Bypass” (Video) ASMBS November 5, 2019
- Tsai C, Zehetner J, Steffen R, “Laparoscopic Conversion from Gastric Sleeve to Roux-en-Y Gastric Bypass with Remnant Gastrectomy using Fluorescent Angiography” (Video) ASMBS November 6, 2019
- Tsai C, Zehetner J, Bally L, Steffen R, “Impact of roux-en-y gastric bypass alimentary limb length on long-term weight loss, diabetes, and dumping syndrome outcomes,” Swiss Surgical Society Congress, Bern, Switzerland May 17, 2019
- Tsai C, Zehetner J, Beel J, Steffen R, “Long-term outcomes and frequency of revisional bariatric surgeries 15 years and beyond after gastric banding: A high band failure rate with safe revisions,” Swiss Surgical Society Congress, Bern, Switzerland May 16, 2019
- Tsai C, Steffen R, Kessler U, Lipham J, Zehetner J, “Post-operative dysphagia following magnetic sphincter augmentation for gastroesophageal reflux disease,” Swiss Surgical Society Congress, Bern, Switzerland, May 15, 2019
- Tsai C, Steffen R, Kessler U, Zehetner J, “Endoscopic gastro-jejunal revisions for treatment of dumping syndrome after Roux-en-Y gastric bypass,” SAGES, Baltimore, MA April 4, 2019
- Tsai C, Zeheter J, “Laparoscopic Hiatal Hernia Repair with Posterior Cruroplasty and Magnetic Sphincter Augmentation in a Patient with GERD and Large Type III Hiatal Hernia,” ACS, Boston, Massachusetts, October 24, 2018 (video)
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Laparoscopic Magnetic Sphincter Augmentation with routine Posterior Cruroplasty: Postoperative Dysphagia and Hiatal Hernia Recurrence,” ACS, Boston, Massachusetts, October 25, 2018 (quickshot)
- Tsai C, Zehetner J, Kessler U, Steffen R, “Long-term results of pancreatectomy for post-gastric bypass hypoglycemia,” IFSO, Dubai, UAE, September 27, 2018
- Tsai C, Zehetner J, “Conversion of gastric banding to laparoscopic sleeve gastrectomy with perfusion assessment using laser-assisted fluorescence angiography,” IFSO, Dubai, UAE, September 27, 2018 (video)
- Tsai C, Zehetner J, “Laparoscopic sleeve gastrectomy with perfusion assessment using laser-assisted fluorescence angiography,” IFSO Dubai, UAE, September 28, 2018 (video)
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Endoscopic gastrojejunal revisions following gastric bypass: lessons learned in more than 100 consecutive procedures,” Digestive Disease Week (SSAT sessions), Washington DC, June 5, 2018
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Endoscopic closure of gastro-gastric fistula after gastric bypass: a technically feasible procedure but associated with low success-rate,” Digestive Disease Week (SSAT sessions), Washington DC, June 4, 2018
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Dumping syndrome after gastric bypass: endoluminal revision of the dilated gastrojejunostomy is a safe and highly effective treatment option,” presented as oral presentation as part of Best Abstracts session at International Federation for the Surgery of Obesity and Metabolic Disorders, European Chapter (IFSO-EC), Athens, Greece, May 19, 2018
- Tsai C, Zehetner J, Kessler U, Steffen R, “Outcomes 15 years and beyond following adjustable gastric banding for morbid obesity: high band failure rate with safe revisions,” IFSO-EC, Athens, Greece, May 17, 2018
- Tsai C, Steffen R, “Re-sleeve with silastic ring and crurorhaphy in a rare case of severe hyperinsulimic hypoglycemia after sleeve gastrectomy,” IFSO-EC, Athens, Greece, May 18, 2018 (video)
Poster Presentations (10)
- Tsai C, Zehetner J, Bally L, Steffen R, “Long-term weight loss, diabetes, and dumping syndrome outcomes after short versus long alimentary limb roux-en-y gastric bypass,” DDW (SSAT sessions), San Diego, CA May 21, 2019
- Tsai C, Steffen R, Zehetner J, “Perfusion assessment using laser-assisted fluorescence angiography during conversion of gastric band to laparoscopic sleeve gastrectomy,” Swiss Surgical Society Congress, Bern, Switzerland May 15-17, 2019
- Tsai C, Steffen R, Zehetner J, “Laparoscopic hiatal hernia repair with posterior cruroplasty and magnetic sphincter augmentation in patient with refux and large type III hiatal hernia,” Swiss Surgical Society Congress, Bern, Switzerland, May 15-17, 2019
- Tsai C, Steffen R, Kessler U, Zehetner J, “Gastroesophageal reflux disease after bariatric surgery: Magnetic sphincter augmentation in patients with normal esophageal motility,” Swiss Surgical Society Congress, Bern, Switzerland, May 15-17, 2019
- Tsai C, Herzig D, Zehetner J, Kosinski C, Kunezli C, Stauffer TP, Nett P, Steffen R, Stettler C, Bally L, “Incretin response in patients with postprandial hyperinsulinemic hypoglycemia following gastric bypass surgery with or without extended distal pancreatectomy,” World Congress on Interventional Therapies for Type 2 Diabetes (WCITD), New York, NY, April 8-10, 2019
- Tsai C, Steffen R, Kessler U, Lipham J, Zehetner J, “Post-operative Dysphagia Following Magnetic Sphincter Augmentation for Gastroesophageal Reflux Disease,” SAGES, Baltimore, April 3 – 6 2019
- Tsai C, Steffen R, Kessler U, Zehetner J, “Gastroesophageal reflux disease after bariatric surgery: magnetic sphincter augmentation in patients with normal esophageal motility,” IFSO, Dubai, UAE, September 26-29, 2018
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Dumping syndrome after gastric bypass: endoluminal revision of the dilated gastrojejunostomy is a safe and highly effective treatment option,” DDW (SSAT sessions), Washington DC on June 5, 2018
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Endoscopic gastrojejunal revisions following gastric bypass: lessons learned in more than 100 consecutive procedures,” European Association of Endoscopic Surgeons (EAES) in London, United Kingdom May 31-June 1 2018
- Tsai C, Kessler U, Merki H, Steffen R, Zehetner J, “Endoscopic closure of gastro-gastric fistula after gastric bypass: a technically feasible procedure but associated with low success-rate,” EAES, London, United Kingdom May 31-June 1 2018
Awards
- Best Video Presentation International Award, ASMBS Obesity Week, 2019
- SSAT Resident and Fellowship session honoree, Digestive Disease Week, 2018
- Best Video Presentation, IFSO, 2018
Saudi doctors learn in Bern
After Dr Jörg Zehetner was able to familiarise a total of five surgeons from Saudi Arabia with the LINX Reflux Management System, a special reflux surgical technique, in the summer of 2019, the next five medical professionals from Saudi Arabia now stood together with the Swiss specialist at the virtual operating table. In a special workshop on the LINX Reflux Management System, the Saudi surgeons were trained in the modern techniques of the procedures. While the summer was spent teaching and training in Saudi Arabia, the November workshop took place in Bern.
Johnson & Johnson had once again selected Dr Zehetner as an expert, who now conducted the workshop lasting several days directly in the Swiss1Chirurgie clinic at Schänzlihalde 1 in Bern. In addition to other special facilities, a meeting room with state-of-the-art presentation and video technology is also available there. In this way, it was possible to clearly and comprehensibly demonstrate and try out how the LINX Reflux Management System is to be applied to patients in need of treatment. Dr. Jörg Zehetner was supported by his colleague Dr. Karl Miller, with whom he has already worked as J&J Faculty at several clinics in Saudi Arabia.
After Dr Jörg Zehetner was able to familiarise a total of five surgeons from Saudi Arabia with the LINX Reflux Management System, a special reflux surgical technique, in the summer of 2019, the next five medical professionals from Saudi Arabia now stood together with the Swiss specialist at the virtual operating table. In a special workshop on the LINX Reflux Management System, the Saudi surgeons were trained in the modern techniques of the procedures. While the summer was spent teaching and training in Saudi Arabia, the November workshop took place in Bern.
Johnson & Johnson had once again selected Dr Zehetner as an expert, who now conducted the workshop lasting several days directly in the Swiss1Chirurgie clinic at Schänzlihalde 1 in Bern. In addition to other special facilities, a meeting room with state-of-the-art presentation and video technology is also available there. In this way, it was possible to clearly and comprehensibly demonstrate and try out how the LINX Reflux Management System is to be applied to patients in need of treatment. Dr. Jörg Zehetner was supported by his colleague Dr. Karl Miller, with whom he has already worked as J&J Faculty at several clinics in Saudi Arabia.
EMEA trainings bring regions together
EMEA is the grouping of Europe, the Middle East and the Americas that Johnson & Johnson has put together specifically to further develop treatments and surgical techniques for reflux disease. At the same time, these are the regions where reflux diseases requiring treatment are becoming more frequent.
As with the training sessions in the two German cities of Speyer and Wiesbaden, the focus of the training sessions was once again on the LINX magnetic ring, which brings decisive advantages for the new treatment technique.
Reflux diseases on the rise
The number of new cases of reflux disease continues to increase in the EMEA regions. Reasons for this include a changed lifestyle with sumptuous food and a corresponding increase in obesity. Even though this is a rather new form of affluent disease in the Middle East, it is still on the rise. Accordingly, it is important to already familiarise the appropriate medical professionals with the current expertise on the LINX Reflux Management System.
Typical signs of chronic reflux disease are frequent acid regurgitation, heartburn and burning in the stomach. The decisive factor here is not the occasional occurrence of such complaints, but a continuous and/or frequent observation of such symptoms with the corresponding sequelae, which can manifest themselves primarily in damage to the oesophagus due to constant contact with stomach acid. Subsequent changes in the mucous membrane of the oesophagus can be the first signs of oesophageal cancer. It is therefore advisable, especially for reflux patients over the age of 50, to have a preventive check-up, which should also be combined with a gastroscopy.
For 20 percent of the Swiss population, this is not an unknown disease, while in the countries of the Middle East, however, similar accumulations can already be predicted now. If you want to learn more about reflux disease, we recommend studying the relevant specialist articles on the Swiss1Chirurgie website or in the Swiss1Chirurgie APP.
More quality in reflux treatment through improved education and training
For Dr. Jörg Zehetner, a faculty member of Johnson & Johnson, it is clear that quality in reflux treatment is primarily a question of the appropriate surgical techniques. Continuing education is also seen as correspondingly important, always focusing on the latest and most successful methods in reflux treatment.
Dr. Jörg Zehetner is one of the most experienced surgeons in this field, both nationally and internationally. Accordingly, it is also the right decision to continue to promote the training and further education of colleagues in Germany, Austria and Switzerland, but also in the USA and in Saudi Arabia, for example, with this professionalism.
Together, J&J and Dr Zehetner are planning about two to three English-language EMEA workshops per year in Bern. In addition, there will be four to five further LINX workshops for German-speaking colleagues, also in Bern. This offer is completed by two to three further training series in Hamburg (at the J&J Institute Norderstedt, the J&J training and development centre) including a masterclass training series. This could at least meet the first major demand for specialised training series on the LINX Reflux Management System.
Half of the world’s oesophageal cancer cases in just one country
With a population of around 1.4 billion (as of 2018) and a size of approximately 9.6 million square kilometres, China is the most populous country in the world and approximately 233 times larger than Switzerland. These incredible figures alone show that this is a country with huge potential in all kinds of areas.
Among the less pleasant statistics is the fact that the People’s Republic of China alone accounts for more than half of all oesophageal cancer cases worldwide. In general, this disease is much more widespread in Asia than in Europe, for example.
The unusually high incidence of oesophageal cancer in China was one of the reasons for holding the 2019 OESO World Congress in Beijing for the first time ever, rather than in Europe or the USA. The OESO is a medical society made up of leading surgeons, gastroenterologists, pathologists, radiologists and other professionals in the field of oesophagus and stomach. Prof. Dr. Jörg Zehetner, who offers a specialised range of services for reflux diseases and bariatrics in Switzerland with the Swiss1Chirugie locations in Bern, Brig and Solothurn, is one of these specialists with high recognition worldwide.
Exchange of experience and knowledge every minute
What was particularly interesting about the organisation of the OESO World Congress in Beijing 2019 was that in the main part, technical presentations were each only five minutes long, each followed by a discussion that was also five minutes long. This gave the opportunity to exchange and discuss a lot of expertise within a short time.
This not only encourages the exchange of scientific expertise and opinions. Ideas for new studies are also conceived quite quickly and compactly in this way and can then be further refined later.
Dr Jörg Zehetner was a sought-after expert
In addition to the lectures and opinion pieces of his professional colleagues, Dr. Jörg Zehetner was also a sought-after subject matter expert. His experience from many years of work in the United States and his specialisation in upper GI diseases were just the right profile for a lively exchange with his colleagues.
Topics such as oesophageal cancer, stomach cancer, reflux diseases and diaphragmatic hernias also played an important role in the professional exchange with colleagues. The interactions and complementarities of bariatric and reflux surgery, especially in operations of the oesophagus, stomach and intestine, are a broad field that did not lack a great deal of attention at this year’s OESO Congress.
In a special lecture, Dr Zehetner addressed the topic of the size of the hiatal hernia and the choice of surgical procedure.
The focus was on selecting the most suitable surgical procedure for the individual. Dr Zehetner, who is the only surgeon in Switzerland who is versed in all currently known surgical procedures in this field, emphasised that decision-making must always take place together with the patient if long-term success is to be ensured. Conventional gastric sleeves, partial fundoplication, variants with partial removal of the stomach, LINX reflux management system (magnetic ring), electrical stimulation with Endostim or the new reflux stop system are a selection of methods that must always be chosen well-considered and based on the patient.
Dr. Jörg Zehetner is one of the world’s recognised experts in the field of diaphragmatic hernia and reflux surgery and has published several articles on the subject. Accordingly, the corresponding lecture was listened to with pleasure and followed attentively.
For Dr. Zehetner, it is important in every case to carefully weigh up every intervention and always make a decision in the best interests of the patient. Sometimes, drug treatment may take precedence, as not every patient is suitable for surgery per se. This decision can only be made in discussion with the expert. In the run-up to this, a good counselling interview, a targeted diagnosis and the prognosis for healing are important stages.
Swiss1Chirurgie, with its locations in Bern, Brig and Solothurn, offers such expertise for all patients undergoing bariatric surgery or therapy for reflux disease, abdominal hernias and similar complaints. You can also find out what Swiss1Chirurgie with Dr Jörg Zehetner can do at www.swiss1chirurgie.ch and, of course, always in personal contact with the medical specialists.
Holidays interrupted – 5 patients successfully operated on
Dr Zehetner from Swiss1Chirurgie is one of the five best surgeons in Europe when it comes to operations on the oesophagus for reflux disease using the LINX system. In Switzerland, he is the undisputed number one in this particular field. As a consultant and preceptor for Johnson & Johnson, he is also available to assist with LINX reflux surgeries in Saudi Arabia.
It was only in July 2019 that the Swiss was called from his summer holiday in Spain to Saudi Arabia to provide the surgeons there with the specialist advice and surgical skills they were looking for in two reflux centres for the LINX Reflux Management System. The missions took place on 28 and 29 July 2019 at Prince Sultan Military Hospital in Riyadh and King Fahd Hospital of the University of Khobar, where a total of five patients were offered the required procedures.
Even though these two reflux centres in Saudi Arabia are already specialised in the surgical treatment of reflux disease, it makes a difference when international luminaries in this field support the procedures with the latest techniques and plenty of experience.
Reflux diseases must be thoroughly diagnosed
The most common symptoms of reflux disease include acid regurgitation and heartburn with chronic value. But these two symptoms alone are not enough to make an accurate diagnosis. A comprehensive clarification of the individual appearance requires a gastroscopy, testing of the oesophageal function and an acid measurement. Only the interaction of several factors makes the diagnosis of gastro-oesophageal reflux disease (GERD) accurate and certain. Then it also depends on the right treatment up to surgical intervention.
Incidentally, this form of reflux disease is not only very common in the western world. This clinical picture is also very widespread in the Middle East, so that more work is being done there on training suitable surgeons and creating appropriate treatment centres. Internationally successful specialists like Dr. Zehetner are in particular demand, especially if they can prove that they have spent at least two years abroad on a fellowship as additional training.
LINX system is currently the best
For the surgical treatment of reflux disease after appropriate diagnosis, the LINX system has proven to be the best treatment method. The LINX system is a ring-shaped chain of titanium-coated magnets that is placed around the end of the oesophagus during laparoscopic surgery. This significantly limits suffering, minimises secondary damage and restores patients’ well-being.
This was also the case during the missions in the summer of 2019 in Saudi Arabia, where, with the help of Dr Zehetner from Swiss1Chirurgie, the surgical procedures were successfully performed by the Arab surgeons.
Prof. Dr. Zehetner greatly appreciates the cooperation with his colleagues from Saudi Arabia.
The expert was particularly impressed by the professionalism, the surgical skills and the outstanding hospitality of the Arab surgeons.
“Hospitality is very important here, you are generously served Arabic food, and the gratitude and appreciation is extremely high.
“The beauty of such teaching assignments is the common language that doctors and health workers all over the world speak with each other: Tolerance towards other cultures, putting the patient first, helping and healing.”
The LINX Reflux System is only offered after extensive clarification. Dr. Zehetner will inform you about the exact operation, the advantages, risks and side effects in one of his consultation hours at Swiss1Chirurgie in Bern, Brig or Solothurn.