Colorectal surgery
In colorectal surgery, we treat benign and malignant diseases of the small intestine, colon and rectum. The Swiss1Chirurgie team has many years of experience as well as a high level of expertise and specialisation in this exciting field.
Operations on the small and large intestine are very common. They may be necessary in the case of intestinal infections – e.g. diverticulitis, appendicitis or chronic inflammatory bowel diseases such as Crohn’s disease or ulcerative colitis.
Bowel surgery is also necessary for large polyps or bowel cancer.
Early detection of intestinal diseases is important so that the necessary therapy can be initiated in time.
How do diseases of the intestine make themselves noticeable?
The symptoms differ depending on the disease. In addition to abdominal pain, an infection often causes a general feeling of illness, fever, diarrhoea or vomiting. With benign and malignant tumours, there is often blood in the stool, changes in bowel movements or even abdominal cramps and vomiting. However, tumours often do not show any symptoms at all.
What are the diagnostic possibilities?
In addition to the conversation with the doctor and the clinical examination of the abdomen, a colonoscopy is often necessary for diseases of the intestine. This should be carried out from the age of 50, even without symptoms, in order to detect and treat possible bowel cancer or the preliminary stages (polyps). If there is a family history of colorectal cancer, a colonoscopy should be performed from the age of 40. Colonoscopy can detect infections, polyps, diverticula and bowel cancer. Polyps can often be removed during the colonoscopy and examined afterwards.
Other examinations of the intestine include ultrasound of the abdomen, computer tomography (CT) or magnetic resonance imaging (MRI). There, infections of the intestine, diverticula or even intestinal tumours can be detected.
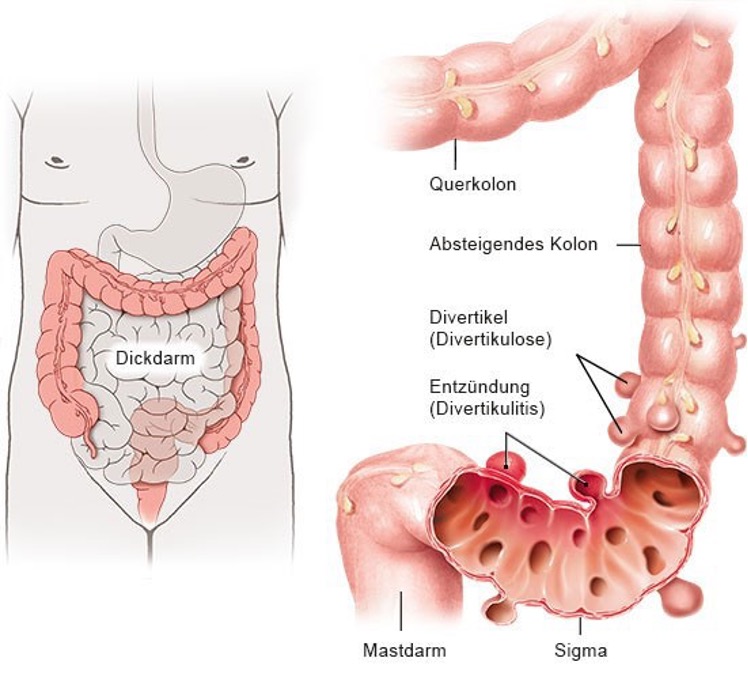
Diverticulum
Diverticula are protrusions of the intestinal wall, they are mostly located in the lower part of the colon, in the sigmoid colon. Diverticula are very common with age – 80 percent of people over 80 have diverticula. Most of them remain symptom-free. Symptoms arise from infections of the diverticula, which is then referred to as diverticulitis.
Uncomplicated diverticulitis often heals on its own or with the help of antibiotics. Complicated infection can lead to perforation of a diverticulum. This can cause an abscess or even stool to leak into the abdominal cavity. Sometimes an emergency operation is then necessary. If antibiotic therapy does not work, surgery is also necessary. After complicated diverticulitis has healed or after several uncomplicated episodes of diverticulitis, surgery of the affected section of the intestine is also recommended.
Polyps and bowel cancer
Polyps are precursors of bowel cancer and are still benign. If they can be removed endoscopically, no further therapy is needed. In the case of a malignant tumour, however, surgery is practically always necessary. Often, however, a cure is possible through surgery.
How is bowel surgery done?
Whenever possible, we operate on the bowel laparoscopically, i.e. using the keyhole technique. This is much gentler than open surgery. In benign diseases, the diseased section of the intestine is removed and the two ends are closed again with a suture. For this we often need a staple gun. In the case of malignant tumours, not only the affected section of the intestine but also the feeding veins and lymphatic channels must be operated on in order to remove all tumour cells.
In the case of tumours far down in the large intestine (rectum or rectum), a temporary artificial anus sometimes has to be created to allow the suture to heal properly.

The removed bowel is always sent to pathology and then examined histopathologically under the microscope. Depending on the stage of the tumour, supplementary chemotherapy (adjuvant therapy) may be needed after the operation. In the case of cancer of the rectum, chemotherapy and/or radiotherapy is sometimes necessary even before the operation (neoadjuvant therapy). This reduces the size of the tumour and increases the success of the operation and the chances of recovery.
All patients with cancer are discussed at our interdisciplinary tumour board. There, the best therapy is determined by all specialists (cancer specialists, radiologists, radiotherapists, surgeons) together.
An operation on the small or large intestine usually takes between 1-3 hours, the hospital stay 3-6 days.
SIMPLY EXPLAINED
Film reports & lectures on acid reflux, oesophageal cancer, aftercare and other medical topics.